Table of Contents
- Common Causes of COPD
- Understand COPD and Its Classifications
- Specific Symptoms and Clinical Findings
- Document Type and Severity of COPD
- State the Presence of Acute Exacerbations
- Note Any Associated Conditions or Complications
- Specify Tobacco or Nicotine Use
- Include Test Results That Confirm COPD
- Long-Term Oxygen Therapy and Interventions
- Use Standard COPD Terminology
- Ensure Documentation Matches the Provider’s Clinical Judgement
- Update Documentation for Each Visit
- Tips to Help Providers Improve COPD Documentation
- Common Mistakes in COPD Documentation
- ICD-10 COPD Documentation Checklist
- Case Study: Turning Poor COPD Documentation into Great Documentation
- Documentation Tips for Specific Settings
- What Auditors Look for in COPD Documentation?
- Conclusion
Chronic Obstructive Pulmonary Disease, or COPD, is one of the most common and serious chronic conditions affecting millions of people worldwide. For healthcare providers, accurately documenting COPD is critical not only for patient care but also for proper ICD 10 coding. Clear and detailed documentation helps coders assign the correct ICD 10 codes, which affects billing, data reporting, and treatment outcomes. To support ICD 10 level of specificity, providers must use best practices that are clear, consistent, and clinically meaningful.
Common Causes of COPD
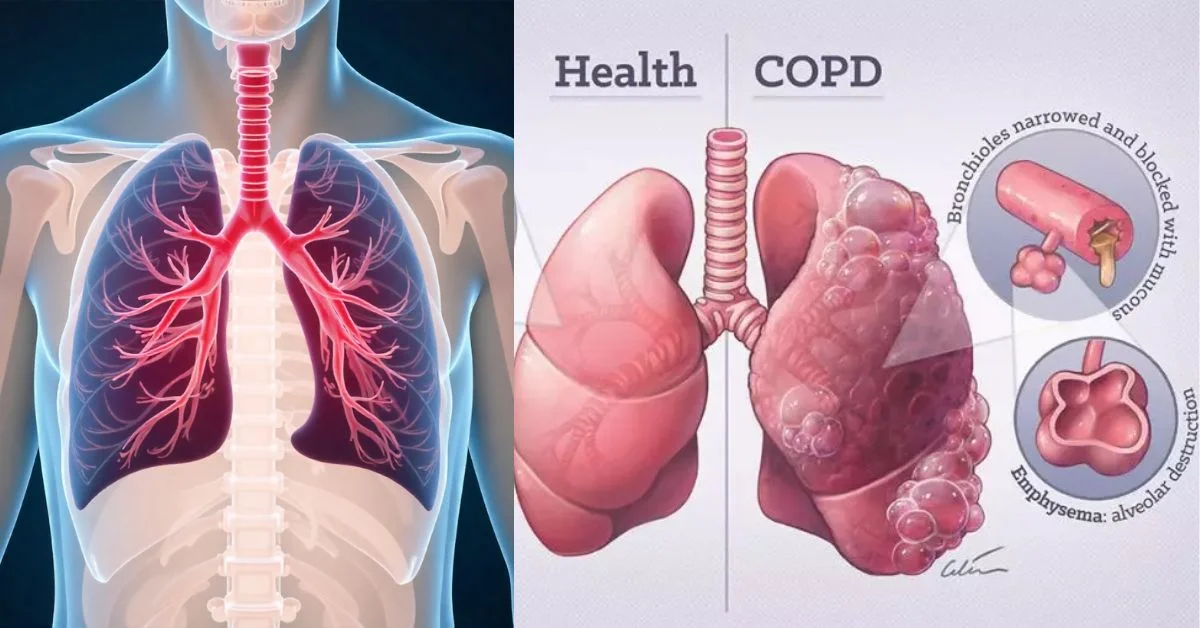
Chronic Obstructive Pulmonary Disease (COPD) is a group of long-term, progressive lung conditions that limit airflow. Most cases develop from prolonged exposure to harmful substances that damage the lungs.
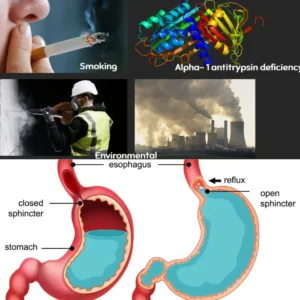
1. Smoking
Cigarette smoking commonly leads to the development of COPD. Years of inhaling tobacco smoke break down lung tissues and inflame airways, making it harder to breathe over time.
2. Environmental Exposure
Long-term exposure to toxic fumes, dust, air pollution, and secondhand smoke often causes the development of COPD. People who work in industrial or construction settings face higher risk due to constant irritant exposure.
3. Childhood Infections
A history of severe respiratory infections in early childhood, like pneumonia or bronchitis, can damage developing lungs. This damage may increase the chance of developing COPD later in life.
4. GERD May Worsen the Condition
Gastroesophageal reflux disease (GERD) can make COPD symptoms worse. Acid reflux may cause further irritation to the lungs, especially during sleep or when left untreated.
5. Genetics Also Influence Risk
A rare genetic disorder, alpha-1 antitrypsin deficiency, can cause COPD even in people who have never smoked. This condition reduces a protein made by the liver that normally protects lung tissue from damage.
Understand COPD and Its Classifications
COPD is a general term, but ICD 10 demands much more precision. Simply writing “COPD” is not enough. The ICD 10 code J44.9 is used for unspecified COPD, but more specific codes are available depending on the condition’s cause, severity, and complications. For example:
- J44.0: COPD with acute lower respiratory infection
- J44.1: COPD with (acute) exacerbation
- J44.9: COPD, unspecified
This classification shows that COPD documentation must cover more than just the name of the disease.
Specific Symptoms and Clinical Findings
When documenting COPD, always include detailed symptoms and clinical findings. This is essential for ICD 10 specificity. Note if the patient has:
- Chronic cough
- Shortness of breath
- Wheezing
- Fatigue
- Cyanosis
- Barrel chest
Be specific about frequency and severity. For instance, say “persistent cough for three months” instead of “chronic cough.” Use descriptive language that clearly paints the clinical picture, helping coders choose the right ICD 10 code.
Document Type and Severity of COPD
A key best practice involves clearly stating the type and severity of COPD. ICD 10 requires this detail to support accurate coding. Types of COPD can include:
- Emphysema
- Chronic bronchitis
- Mixed COPD
You should also include severity based on clinical judgment, spirometry results, or GOLD classification. Clearly identify whether the COPD is mild, moderate, severe, or very severe. Include FEV1 percentage if available.
Example: Document it as: “The patient has moderate COPD (FEV1 between 50% and 80%), with a mixed type and frequent exacerbations.”
State the Presence of Acute Exacerbations
COPD exacerbations involve sudden flare-ups or worsening of symptoms. This detail matters because ICD 10 assigns a specific code (J44.1) for acute exacerbations. If a patient comes in with increased coughing, wheezing, or shortness of breath and needs immediate care, document it clearly.
Example: “The patient reports an acute COPD exacerbation with worsened shortness of breath, increased sputum production, and wheezing over the past 48 hours.”
Detailed documentation like this ensures accurate ICD 10 coding and guides appropriate treatment planning.
Note Any Associated Conditions or Complications
Often, COPD does not appear alone. It’s common to see it alongside other respiratory conditions or complications. Always document if the patient has:
- Asthma (J45 codes)
- Pneumonia (J18 codes)
- Pulmonary hypertension (I27 codes)
- Respiratory failure (J96 codes)
- Heart failure
For example: “COPD with acute lower respiratory tract infection and acute hypoxic respiratory failure.” This level of documentation allows coders to capture all aspects of the patient’s condition and ensures that billing reflects the complexity of care.
Specify Tobacco or Nicotine Use
Smoking history is a major part of COPD documentation. ICD 10 provides specific codes for:
- Current smoker (F17.2)
- Former smoker (Z87.891)
- Exposure to environmental smoke (Z77.22)
- Counseling for tobacco use (Z71.6)
Clearly state if the patient currently smokes, has quit or never smoked. Also, include how long they smoked, how many packs per day, and the number of years. For example:
“40 pack-year history; quit smoking 3 years ago.”
ICD 10 coding and risk adjustment rely directly on this information.
Include Test Results That Confirm COPD
Clinical documentation should include the diagnostic tools used to confirm COPD. The most common is spirometry. Document values like FEV1, FVC, and the FEV1/FVC ratio. Also, mention imaging results such as chest X-rays or CT scans that support the diagnosis.
Example: “Spirometry confirms airflow limitation with FEV1 45%, FVC 65%, FEV1/FVC ratio <70%. Consistent with severe COPD.”
This practice supports coding accuracy and shows that the diagnosis is evidence-based.
Long-Term Oxygen Therapy and Interventions

If the patient is on long-term oxygen therapy, make sure this is documented. ICD 10 uses the code Z99.81 to represent dependence on supplemental oxygen. Also include other interventions like:
- Inhalers and bronchodilators
- Pulmonary rehabilitation
- Steroid use
- Nebulizer treatments
Example: “Patient uses supplemental oxygen 2L/min via nasal cannula 24/7, on tiotropium inhaler and albuterol nebulizer.”
These details help support medical necessity and guide both coding and care planning.
Use Standard COPD Terminology
Avoid vague or outdated terms when documenting COPD. Instead, use language that matches the ICD 10 system and clinical guidelines. Avoid using terms like “smoker’s lung” or “chronic chest condition”; use accurate clinical terms instead.
- “Chronic obstructive pulmonary disease”
- “Chronic bronchitis”
- “Emphysema”
- “COPD with acute exacerbation”
Using precise and consistent terms ensures your documentation supports ICD 10 specificity and avoids confusion during coding.
Ensure Documentation Matches the Provider’s Clinical Judgement
Your documentation must always reflect the provider’s assessment and decision-making. Don’t just list symptoms; link them to the diagnosis. If you list shortness of breath, you should explain if it is part of COPD or another condition.
For example:
“Shortness of breath due to acute COPD exacerbation, worsened by recent upper respiratory infection.”
This ensures the medical record supports both the diagnosis and the coding, and protects the provider during audits.
Update Documentation for Each Visit
COPD is a chronic condition, but it can change over time. That’s why it’s important to update the documentation during each patient encounter. Note any:
- Changes in symptoms
- Medication adjustments
- Hospitalizations or ER visits
- Pulmonary function test updates
- Changes in oxygen needs
Keep the documentation current. Stale or copied notes can lead to incorrect coding and poor patient care. Even if the patient seems stable, include a brief status update like:
“Patient remains stable with no recent exacerbations. Continues current medication regimen.”
This builds a strong clinical story and allows coders to assign the right ICD 10 code for that date of service.
Tips to Help Providers Improve COPD Documentation
Use these real-world tips toward better documentation
1. Educate with Templates & Smart Phrases
Use EMR templates that prompt for specific COPD types, exacerbation status, and complications. Smart phrases can cut down on typing and improve clarity.
2. Clarify Terms: Avoid Ambiguity
Avoid vague terms like “history of COPD” when referring to an active condition. Instead, write “patient with known COPD, currently stable.”
3. Don’t Rely on Pulmonary Function Tests Alone
PFTs may show obstruction, but clinical documentation is required to support the diagnosis. Always document symptoms, treatment plans, and assessments.
Common Mistakes in COPD Documentation
Some frequent errors that trip up providers and coders alike.
Mistake 1: Missing Exacerbation Details
Saying “exacerbation” without describing symptoms leaves the coder guessing.
Fix: Always describe the acute symptoms and treatment.
Mistake 2: Not Mentioning Tobacco Use
ICD-10 requires a clear status: current smoker, former smoker, or never smoked.
Fix: Add tobacco history in the social history section or directly in the assessment.
Mistake 3: Using “COPD” as a Blanket Term
Lumping chronic bronchitis, emphysema, and COPD together without distinction leads to generic codes.
Fix: Be specific every word counts in documentation.
ICD-10 COPD Documentation Checklist
Here’s a quick cheat sheet you can use:
- Specify type (chronic bronchitis, emphysema, ACOS)
- Indicate if stable or exacerbated
- Note any lower respiratory infections
- Document related conditions (e.g., heart failure)
- State smoking status
- Avoid vague terms
- Use supporting terms (dyspnea, wheezing, etc.)
Print this and keep it near your workstation. Consistency is key.
Case Study: Turning Poor COPD Documentation into Great Documentation
Before (Poor):
“Patient with COPD, on inhalers. Comes in for a refill.”
After (Improved):
“72-year-old male with emphysema-type COPD, stable on tiotropium and albuterol. No signs of acute exacerbation. Non-smoker since 2015. Denies cough, fever, or sputum changes.”
Why It’s Better:
- Type specified (emphysema)
- Status clarified (stable)
- Medication noted
- Smoking history added
- Symptoms reviewed
This version supports the code J43.9 (emphysema, unspecified) plus Z87.891 (history of tobacco use).
Documentation Tips for Specific Settings
Inpatient Setting
Include severity, respiratory support (like oxygen), and comorbidities. Make sure to capture all present-on-admission diagnoses.
Outpatient Clinics
Note if this is a follow-up, new diagnosis, or acute visit. Clearly document the plan of care and medication management.
Emergency Department
Emphasize acute symptoms and interventions (e.g., nebulizer treatments, steroids). Clarify if it’s a new or known COPD diagnosis.
What Auditors Look for in COPD Documentation?
If your charts are ever reviewed by payers or compliance teams, here’s what they’ll expect to see:
- Precise ICD-10 alignment
- Symptom and treatment match
- Medication reconciliation
- Status of disease (stable vs. exacerbated)
- Clear links to contributing factors (like smoking)
Documentation that doesn’t support the code = risk. Avoid this by always telling the full clinical story.
Conclusion
Documenting COPD to support ICD 10 level of specificity is essential for accurate coding, proper reimbursement, and high-quality patient care. Providers must focus on including the type of COPD, the severity, any acute exacerbations, complications, smoking status, and relevant test results. Keeping documentation detailed and up to date ensures it tells a clear and correct clinical story. Following these best practices not only helps meet regulatory requirements but also improves outcomes for patients living with COPD. Proper documentation is not just about coding it’s about delivering safe, effective, and efficient care every step of the way.













